The Practice Success Prescription: Team-Based Veterinary Healthcare Delivery by Drs. Leak. Morris Humphries
Thomas E. Catanzaro, DVM, MHA, FACHE, DACHE
"The best way to begin, is to begin."
The change from a one-doctor, one or two-examination/consultation room system, to a two-doctor system is usually minor. The owner just takes more time off. We usually find that the two doctors just divide the longer one-doctor shift into two, continue to work in the traditional linear fashion, and never give it another thought.
When a practice moves beyond two doctors, beyond nine hundred transactions a month, or when they expand into five or more consultation rooms, there are psychological, physical, and problematic issues to address in the basic operating premises.
The practice style of two doctors, working two or three consultation rooms, flowing erratically front to back, cannot be done in a practice that doubles in size. Zones must be established in a larger facility. To concentrate the doctor resources on the client needs the nursing staff must concurrently accept veterinary extender roles.
The need for an odd number of outpatient rooms becomes evident below.
| Figure 14: Zones Systems | 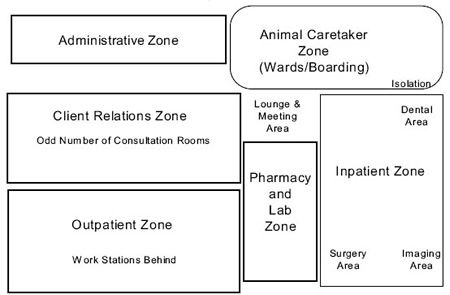
|
|
| |
Sample Zoning of a Veterinary Facility
Developing hospital zones, initially as "client relations", "inpatient, and "outpatient", and maybe later, "resort" and "surgery", requires the client relations (reception) team and nursing (technician) staff to accept accountability for zone operations, and see the doctors as visiting consultants. This means the doctors work a specific zone for only a half day, then shift zones.
The team-based, client-centered, scheduling, and multi-tasking team techniques (mt3), is based on staff proficiency in wellness practices, but can be tailored to specialty practices as well, such as effective use of triage nurses in an emergency/critical care practice. Shift changes occur only after/when all restocking and cleaning is completed, or the shortfalls are transferred in an overt and apologetic manner. Caution: this all occurs as the only after Phase Five training has been completed, as shown in Appendix D of this text, as well as the VCI® Signature Series Monograph, Zoned Systems & Schedules.
|
Clarification
The VCI® Signature Series Monograph Staff Orientation & Training has been designed as self-directed training for the individual, and soon to be available in high speed access streaming video. The VCI® Signature Series Monograph Zoned Systems & Schedules has been designed for coordinated team development.
If the practice has not embraced the synergy model shared in Chapter One, and if there is not recurring training planned into the practice's weekly flow, it will be a rare practice that can achieve the entire program. We believe the staff must be trained to a level of being trusted within their respective zones, and receive recurring continuing education to maintain the cutting edge of excellence. |
The problems associated with doctor-centered healthcare delivery exist because this is how most all veterinarians are trained in school, so it is how they start their practices. These problems can now be addressed by staff at shift change, from updated medical records and charge sheets (travel sheets), to restocking and cleaning. In short, the goal is for the staff to leave the hospital zone in better shape than they found it. Below, the term "about" or "usually" are used for practice-specific decisions, or community demand variables. It is critical to understand that while these principles are time-proven, the tailoring to individual practice environments is also critical, and in fact, is what Veterinary Consulting International® (VCI®) does as a key part of their consulting assistance to companion animal and mixed animal veterinary practices:
 An Outpatient Nurse Technician (OPNT) "usually" controls at least two consultation rooms, formerly called exam rooms, one outpatient doctor, and shares one pharmacy technical assistant float.
An Outpatient Nurse Technician (OPNT) "usually" controls at least two consultation rooms, formerly called exam rooms, one outpatient doctor, and shares one pharmacy technical assistant float.
The Inpatient Nurse Technician (IPNT) "usually" controls treatment, surgery, and radiology, "usually" one inpatient doctor, and one inpatient technical assistant float, as well as "usually" overseeing the animal caretaker staff, who may act as technical assistants, when ward occupancy is low.
The physical location of the laboratory most often determines who has operational control of that zone, and the potential staffing.
Morning outpatient appointments are scheduled from "about" 7:30 a.m. to 12:30, so the outpatient team (explained later) can leave the zone by 1:00 p.m.. The afternoon outpatient shift is from "about" 12:30 to 5:00 p.m., and the evening outpatient shift (on practices with "late days") is "about" 4:00 to 8:00 p.m. This evening doctor usually starts the shift with OHE and neuters from noon to 3 p.m., and then has "about" 3:00 to 4:00 p.m. for food and phone calls.
Morning inpatient nursing rounds are at "about" 7:30 a.m., which means all cases are "usually" prioritized by the IPNT on the treatment room white board before 8:00 a.m., and at 8:00 a.m. the doctor "usually" validates the plan with the morning IPNT. The IPNT may ask the doctor to review a few of the atypical cases that need doctor evaluation.
The morning outpatient system stops at "about" 12:30, and the afternoon inpatient rounds occur at "about" 1:00 p.m.. That means there are thirty minutes to overtly transfer the shift to the next team, and an additional nursing round is conducted.
The afternoon inpatient priority changes are based on RTG (ready-to-go) times, so when the doctor reviews the cases, which have been prioritized by the IPNT, the promises made to the clients are foremost in the their minds.
Morning outpatient staff "usually" becomes the afternoon inpatient team, so they can ensure their "day admits" are closed out as promised. The morning inpatient team "usually" becomes the afternoon outpatient team, so they can ensure they are available if there are questions at inpatient discharge. The noon to 8:30 p.m. doctor shift allows a larger practice the high-density scheduling overlap for end-of-day rush times, common in bedroom communities and high, dual-income populations.
In some cases, there is a doctor or nurse/technician who has no client relations skills, and must be relegated to the inpatient zone. While this sounds like a premium medical/surgical situation, it reduces the person's effectiveness for the practice, and, therefore, the person cannot leverage his or her own earning potentials. Most employers limit the compensation if people are less flexible in supporting the practice's mission.
The evening transfer of zones is "usually" assumed to be similar to the day exchange, and assessed by the morning shift. It may require greater calibration coordination, but the habits built on the midday shift change between zones will eventually carry over to EOD changes.
The key elements to accept in this transition of thought include:
 No one leaves one's zone during the shift, including doctors, except for the technical assistants, who are moving animals.
No one leaves one's zone during the shift, including doctors, except for the technical assistants, who are moving animals.
The nursing staff has accountability for maintaining the client/patient-centered schedule and keeps the doctors on schedule.
The doctors must respect the schedules and the nurses.
The hospital's consultation rooms, tables, suites, and facilities are scheduled, not the doctors, with a client-centered commitment to the social contract of meeting the clients' expectations in a timely manner.
The ability to tailor the above to a specific practice, with specific human resources, and a specific client base has always been the focus of VCI®. Please remember our original thesis: all veterinary practices have the staff they deserve, and after twenty-four months of operation, have the clients they deserve. These are the ones they attracted and maintained in both cases. The staff has always been trained in the doctor's image, so the problems in the staff are actually leadership challenges in effective training, inviolate core values, standards of care, or mission focus. Just look in the mirror. You have met the enemy, and they are us!
|
Multi-Tasking Team Techniques (mt3)
In the initial days of our sharing the VCI®, principles of team-based veterinary healthcare delivery, the term "high-density scheduling" came to the forefront. Because we were changing from the linear format, so commonly learned from the veterinary teaching hospital, or the habits learned from ambulatory medicine farm calls, the traditionalists tagged staff-based healthcare delivery as "high-density" rather than "multi-tasking", or "doctor leveraging".
The principles of multi-tasking team techniques (mt3) have been well established in dentistry, optometry, and human healthcare delivery, even for podiatrists and chiropractors. These team-based delivery principles have proven to be very effective for leveraging the primary care givers' time/availability/impact, and concurrently, greatly increased the profitability of the professional practice. Moreover, the use of provider extenders has not deteriorated the quality of care the patient receives, and in most cases, increased the responsiveness and completeness of care.
The actual experience in veterinary medicine has been that team-based, client-centered, scheduling and multi-tasking team techniques (mt3), has been the hallmark difference between less than $450,000 per FTE doctor of a linear scheduling habit, to more than doubling that FTE doctor's income production, still within a normal, forty-hour work week. |
The most effective scheduling is usually done by computer, and most of the newer computer programs like Cornerstone, Avimark, Impromed, ClientTrax, WINVET, DVMax, etc., have been developing good clinical appointment capabilities, with variable boarding capabilities. The secret to adapting the computer program is that a scheduling column is a consultation room, never a doctor/person.
For example, the first column is the doctor's name for the hours on outpatient shift, and the second and third columns will be consult rooms number one and number two. Leave a space column, then show surgery, inpatient, etc., again preceded with a column, showing the doctor's name on the inpatient shift. The doctors request appointments via the OPNT to the client relations (reception) team. Doctors do not touch/adjust the appointment system in any manner. The doctor's inpatient time, besides for telephone voice mail review, can also be a flexible healthcare delivery time, if no surgeries are scheduled. When the outpatient team is fully booked, the inpatient team handles all of the walk-ins, emergencies, and drop-offs through an "odd" consultation room.
In the slow season, only one of the two consultation rooms assigned to an outpatient doctor needs to be scheduled, and walk-ins, drop-offs, and emergencies can then be used to fill the second room. This is the same system being used with Internet appointments. Clients select their preferred time in one room, while the practice schedules clients on the "seams" in the other room. This will be explained in "high-density scheduling" later in this chapter.
If the two rooms are totally booked for a doctor/OPNT team, the IPNT team will see the walk-ins, drop-offs, and emergencies through the "odd" room, assuming there are an odd number of consultation rooms, and two rooms dedicated per outpatient team, as well as be used to "catch up" an outpatient doctor who has gotten off pace. This is coordinated by the OPNT and the IPNT through reception.
As far as facilities are concerned, we helped design a breakthrough, multi-tasking, consultation room system, with a very tight central nursing node, and the consultation rooms wrapped around in a two hundred seventy-degree arc. It also has an additional discharge/comfort room system directly off of the inpatient zone. This design was used as an example in the text Design the Dream, which is a primer on the control, direction, and monitoring of the architect and construction teams during veterinary facility development. The breakthrough outpatient flow could only be done because the owner understood the economies of scale offered by team-based, client-centered scheduling and multi-tasking team techniques (mt3).